Why I felt compelled to write and share my thoughts and feelings with you…
I am a Southern Black cisgender woman physician scientist, with board certification in Obstetrics and Gynecology, who pursued medicine with the intention and motivation of achieving race and gender equity and inclusion in medicine and healthcare for Black poor women and girls in urban. Along the way, omission and oppression met me in unimaginable, intricate and complex ways that were neglected in my formal medical and academic education and training. Survival of the fittest took on an entirely new meaning. Instead, I found safety, visibility, affirmation, and community in the sexual and reproductive justice and youth empowerment movements. Likewise, my career trajectory shifted to the path of public health, examining and facilitating the health and well-being entire populations. Thus, I relocated from the Midwest and accepted a STD Fellowship in California. Well, the past year of fellowship experiences reminded why and how health care, medicine, research and, at times, public health remains unsafe spaces for persons and communities who look like me.
My two-week summer experience in Seattle attending the 24th Annual Principles of STD/HIV Research raised many critical and compassionate questions about the role and responsibility of public health in STI/HIV research, clinical Practice, and health care services and systems change. I want to share context: the audience is composed of the individuals and groups from diverse disciplines including but not limited to health care, medicine, research, programs, epidemiology, and basic sciences, from various academic institutions, state and federal public health agencies, community based organizations, and public health and medical laboratories from various states and regions within the United States and countries from around the world. Each year approximately 60-80 persons attend this course, which seems to serve as a rite of passage for persons with early or emerging careers in or related to the field of STI/HIV research.
Recently, I provided a summary of my experiences in the form of presentation entitled, Observations & Implications: Lived Principles of STD/ HIV Research. That presentation naturally transitioned in the thoughts and feelings I decided to share with you in my first blog entry.
As public health professionals in relationship with researchers, health care providers/systems, and the public:
- What is our collective vision?
- What are our respective and mutual values and goals?
- What is our common language and framework by which we all communicate and collaborate with one another?
- How do ensure that our shared values, practices, and polices continuously move us all towards diversity, inclusion, and equity
- What is the role and responsibility of public health leadership in informing research and health care vision, goals, strategies, evaluations, and reporting?
- Who among the three – public health, research, and health care – leads in community engagement, development, and empowerment?
When I reflect on the representation of the researchers who presented their and other’s work, in comparison to those in the role of course leadership, organizers, participants, and representation of research subjects – serious concerns about diversity, inclusion, visibility, and power plagued my mind and spirit daily during this course particularly as I listened to the language, illustrations, and reasoning utilized and disseminated by many of the leading experts in this field. And I thought of my own experiences in public health and research during my first year here in California. I began to wonder how much critical and compassionate analysis and occurs in this work particularly at the level of the principal investigator, researcher, epidemiologist, study design team and even the Internal Review Board, to consider how multi-level factors with reciprocating and overlapping interactions drive and/or inform research questions, selection of key population, study setting, identification of variables, methods, analyses, interpretation of results, inferences, and definitions of adherence and compliance.
At the intersections or connections of who we are, how we see and interact with the world and how the world sees and interacts with us, how mindful are we about the impact of the various multi-level and related factors. In the image below, I share the Diversity Wheel which provides a framework and reminder for the diversity each of us brings to our profession and vocation, particularly the fields of public health, research, and health care.
The Diversity Wheel, adapted from Marilyn Loden Workforce America, 1991
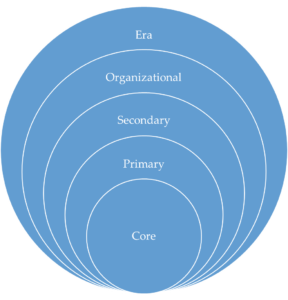
Primary factors such as our physical and mental ability, age, ethnicity, ace, nationality, sexual orientation, and gender continue to inform our lived experiences, values, attitudes, behaviors, communications, interactions, relationships and responses to internal world and external world. Secondary factors such as our relationship/marital status, geographic location, recreational habits, religion, work style, income, personal habits, language including accents and code switching, work experience, family/parental status, and educational background further add to the multiplicity and complexity of our dynamic identities, roles, and responsibilities in and outside of the work place. Organizational factors including not limited to role/job title, work content/field, seniority, work location, and management status further shape our workplace ideas, visions, goals, expectations, relationships, interactions, performance, and satisfaction. Last, not least, Era such as world events, political events, historical moments, social events, and cultural events likely play in an initial and ongoing impact on our workplace knowledge, attitudes, skills, abilities, preferences, and capacities.
At what point in our formal and informal education and training or in every day practice do we ask researchers or ourselves:
- What informs your perspective and approaches to your work in public health? Why are you doing this work?
- What do you hope to achieve?
- How do your personal ambitions, motivation, and/or intentions lead research, public health, and health care closer to diversity, inclusion, and equity?
Word Cloud of My Values
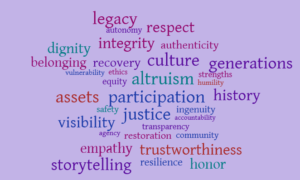
Based upon the mosaic intersections of my identities, roles, responsibilities, skills, knowledge, abilities, and relationships, I identified values listed in the above Word Cloud that are important to me because they shape my perspectives, characterize my intention and motivation to do this work, and inform HOW I approach this work.
I am a Black cisgender woman raised in poverty in the southeastern states in a single black female head of household (remember the stigma and shame of the welfare queen) who managed to experience upward socioeconomic mobility as a result of my education and vocation. AND as an empath and activist, I remain committed to justice, equity, ethics, integrity, and altruistic ingenuity. Thus, I struggled daily during this course as I saw gaps in and opportunities for improved connections and engagements between the lived experiences of the researchers and stories of the populations in which they have studied, built their careers and established their livelihood, legacy, and reputation. Yet again, my mind and heart raised many more critical and compassionate questions about the values, motivations, and intentions of the researchers:
- But who benefits the most from this work?
- Whose needs, priorities, and concerns are centered in the decision making conversations about allocation and distribution of resources, funding, training?
- How authentic and relevant are the research questions, study design, variable selection, and analysis to the needs of the research subjects and the partners, families and communities they represent?
- How do the research interpretations and implications honor and dignify populations under “examination” or “surveillance”?
- What story does our data tell about the history, trauma, resilience, and resistance of the “target” community?
- How does our research characterize the visibility and vulnerability of marginalized communities as both subjects AND co-researcher/principal investigator (PI)?
I found myself wanting to ask each researcher: what is the legacy of your work and who are you mentoring, sponsoring, and developing to move this work forward in a radically responsive, transformative, restorative, and forward thinking way?
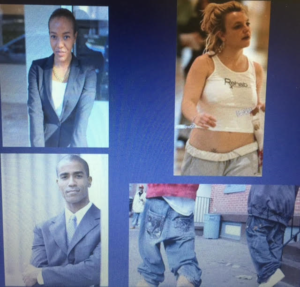 During the one of the lectures, a leading STI researcher and expert incorporated the images to the left in a her presentation on “Writing and publishing peer-reviewed manuscripts”. If you are familiar with me and my career goals, then you know I was initially super psyched about this lecture. She shared insightful information about the what o do and what not to on the path to manuscript writing and publication. Then she wanted to make a point about manuscript errors and writing issues by utilizing the above images, in the following manner, and I paraphrase using the language from an email I sent to my mentor after walking out this specific lecture:
During the one of the lectures, a leading STI researcher and expert incorporated the images to the left in a her presentation on “Writing and publishing peer-reviewed manuscripts”. If you are familiar with me and my career goals, then you know I was initially super psyched about this lecture. She shared insightful information about the what o do and what not to on the path to manuscript writing and publication. Then she wanted to make a point about manuscript errors and writing issues by utilizing the above images, in the following manner, and I paraphrase using the language from an email I sent to my mentor after walking out this specific lecture:
“This what researchers in Africa look like“ [images on the left – see a Black woman and Black man in suits in the top as her BEFORE photos – showing the researchers perceptions of what “researchers in Africa look like”]. “This is what I see when I read their manuscripts with errors“ , displaying images on your right [Black Woman researcher in a suit coat now transformed into a pop culture icon during a challenging time in that person’s life and a Black Man in suit and tie transformed into a Baggy jean pants, hoodies, and Tims wearing inner city thug.] Yes, this is what a lecturer said during this course at 9am. This is not the first time things discriminatory language was used based on age, gender, race, and nationality. These science and research spaces ARE not safe.
When I walked out, I realized I had become the “angry Black woman” again, despite the gross explicit race based and racist language and images being utilized and disseminated in a lecture of higher learning. I just expressed myself very calmly and articulated how this course violated my values of ethics equity justice and safety to the course director and coordinators. I stated she is not the first lecturer to shame and stigmatize Blacks and Africans. And I refused to listen to her for the remaining 9am lecture and her 10am lecture. I found a quiet place to contact my husband and friends for support and validation.
The differences between public health and basic science/clinical approaches to research are striking. I am confident we would have organized a better conference on public health approaches to program, science, and community engagement in STD prevention. Hope the afternoon gets better. Thanks for listening.
Characterization of Young African Women’s Uptake and Adherence to Vaginal Anti-Retroviral (ARV) Ring
- Adherence
- Agency & Autonomy
- Authenticity & Visibility
- Relevancy & Responsiveness
- Sex Positivity to Sex & Sexuality
- Youth Based Participatory Research And Evaluation
A second example of the disconnect between researcher and study subject, particularly at the intersections of gender, age, nationality and race is a researcher’s characterization of African (and not the exact countries in which she studied) adolescent sexuality and her approach to describing why young women did not utilize the vaginal microbicide despite the value and benefit of having access to a highly effective HIV prevention method. I engaged the researcher by asking questions openly during her talk and privately when she approached me directly while sitting at my desk.
Let’s start with adherence:
- What does that mean really?
- Regardless of the scientific proven efficacy of a treatment, what is the most authentic, culturally responsive and humble way to define adherence based on the perspective of the researcher, the science, the methodology, or within the context of the lived experience of the community , study population or study subjects.?
I asked if she planned to incorporate young African women in the planning phase, recruitment, retention, product design, messaging, and imaging, and possibly implementation, evaluation, and dissemination.
I then asked her if she planned to incorporate peer to peer conversations about sex positivity stigma and shame. She said she is not funded to engage her young African women subjects in specific conversations about sex positivity, body image, touch, and self pleasure. I respectfully continued to ask more “accountability to youth centered approaches” in research by asking how she plans include and evaluate youth agency, autonomy, and engagement.
I then raised another yet “unspoken” critical and compassion question to myself. What if the funders may not want to see utilization of vaginal ARVs to increase among youth since youth have sex for many reasons including pleasure, or not necessarily or primarily for romance/love or reproduction? Thus, researchers and public health messages and approaches would have to more diverse and inclusive of a broader range of sexual intentions, motivations and behaviors in order to increase youth engagement and responsiveness. Realizing I am still “inside my head”, I re-engage the researcher lecturer and ask:
- But what are young African women’s intentions and motivations to have sex?
- What are their customary approaches to sex and STI/HIV and pregnancy prevention?
- What does current data say about the uptake and adherence of the contraceptive ring among adolescents in the US or the world, particularly in the African counties in which the researcher lecturer is scaling up vaginal ARV.
- As this baseline information could have served as baseline prevalence for the expected uptake and adherence of vaginal ARV. Likewise, this type of data may offer insight as to whether a ring delivery system works well in youth, who may, for many reasons, have sex and body negative cultural contexts and behaviors that would deter the use of a ring delivery system.
The researcher lecturer responded by affirming the presence of current data on the uptake of the contraceptive ring in the particular country in question, but she either did not know or have the data results immediately accessible to her. Luckily, one of the researchers (likely from that particularly) spoke up and shared the uptake of the contraceptive ring in the particular country is similar to the uptake of ARV ring in the researcher’s study. With that knowledge being shared, then the researchers lecturer agreed the best practice would be NOT to judge young African women for poor utilization and adherence to life saving drug in vaginal ARV, but perhaps to consider a different, more gender, culturally and age appropriate and responsive ARV delivery, in partnership with youth.
What happens when the research subject becomes the PI?
Overall, I found myself questioning the ethics, intention, and relevancy of many methodologies utilized and inferences made, particularly about young women in the US and Africa. I continue to critically and compassionately examine my overall experience, purpose, and place in science, medicine, healthcare, research and public health.
I remain committed to dissemination and implementation research and systems level change. Likewise, I want to serve as a mentor to women, youth, and persons of color interested in science technology engineering arts math and medicine. However, I am not quite sure whether or not the ivory tower of academia or public health academia, local, state or federal agency, or a think tank will allow for safer, more affirming and more authentic spaces or relationships.
The invisibility is pervasive and palpable.
Yet, I do believe investment in qualitative and mixed methods research, public health digital storytelling, and community based participatory research and evaluation are promising strategies to increase community or research subject authenticity, engagement, belonging, visibility, and agency.
Present day, I am coming to the close another educational chapter in my life, with completion of my time in the STD Fellowship in 26 days (but who’s counting.) My hope is to center the voices and lived experiences of women, girls, and youth of color in development, monitoring, and evaluation of community based programs, health service delivery models, and health care provider education and training. I am committed to advancing the fields of sex/gender life science and sexual health by adapting current and/or developing new theoretical frameworks and assessments, instruments, and evaluation tools to better evaluate both provider AND patient comfort, confidence, and behavior during sexual health and STI/HIV prevention visit.
As a result of my 15 month long experiences in California, within the broader context of my experiences in medicine, healthcare, research, and public health, I choose me, myself, and I to center my voice and experiences within my own sister sanctuary, filling in the many pieces that were missing my in mosaic.
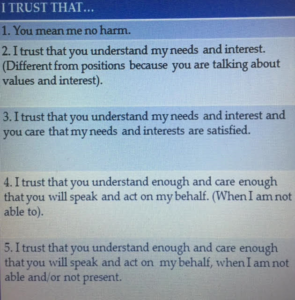 I leave you with a set of expectations and framework around TRUST, by Dr. Louise Diamond Peace Keeper that I believe, if applied consistently and wholeheartedly, we will be better able to center the community, particularly those of us most vulnerable to sexual health and STI/HIV inequalities, inequities, and disparities, in our work as public health professionals in shared spaces and relationships with researchers and health care providers and systems.
I leave you with a set of expectations and framework around TRUST, by Dr. Louise Diamond Peace Keeper that I believe, if applied consistently and wholeheartedly, we will be better able to center the community, particularly those of us most vulnerable to sexual health and STI/HIV inequalities, inequities, and disparities, in our work as public health professionals in shared spaces and relationships with researchers and health care providers and systems.
Through Mosaic Intersections, I invite you to remain curious, compassionate, and critical as we explore race, gender, sex, age, and trauma in policies, programs, and practices in public health, health care, and research.
Until we meet again, thank you.
Scotty
Karen A. Scott, MD, FACOG, Principal & Founder, Mosaic Intersections
Very good an insightful article thank you so much for bringing such wonderful perspective. I have responsibilities for Health and Wellness in the largest company in the world would love to chat with you a bit more about how can we help to change things
You can also reach me on my Walmart email address which is Gloria. Diaz at wal – Mart.com
Greetings, Gloria. Wow!! I greatly appreciate your feedback. I will be contacting you today. Thanks, Scotty.
There’s definately a lot to learn about this subject. I like all the points you’ve made.